Axillary Management After Neoadjuvant Chemotherapy in Node-Positive Breast Cancer
An umbrella review of 23 systematic reviews (13 ELIGIBLE + 10 BORDERLINE) — 2006–2026 with PICOS triage, AMSTAR-2 quality appraisal, PRISMA 2020 reporting, and GRADE certainty assessment. 10 SRs additionally documented as PICOS-excluded with rationale.
Cervera S¹, Duque D², [Biostat³], [Senior Breast Surgeon⁴]. Manuscript ready for submission · Target journals: BJS · EJSO · The Breast.
Cifras del análisis
Abstract (BJS · 250 words)
Background. Axillary management after neoadjuvant chemotherapy (NAC) in clinically node-positive (cN+) breast cancer has evolved from routine completion axillary lymph node dissection (ALND) towards selective omission when nodal pathological complete response (ypN0) is documented by minimally invasive techniques. ≥30 systematic reviews on the topic have produced overlapping but not fully convergent recommendations.
Methods. Umbrella review per JBI methodology and PRIOR-O reporting. PubMed/MEDLINE, EMBASE, Cochrane CDSR and Epistemonikos searched 2006-01 to 2026-04. Independent dual screening and extraction. Methodological quality with AMSTAR-2; reporting with PRISMA 2020; certainty per outcome with GRADE.
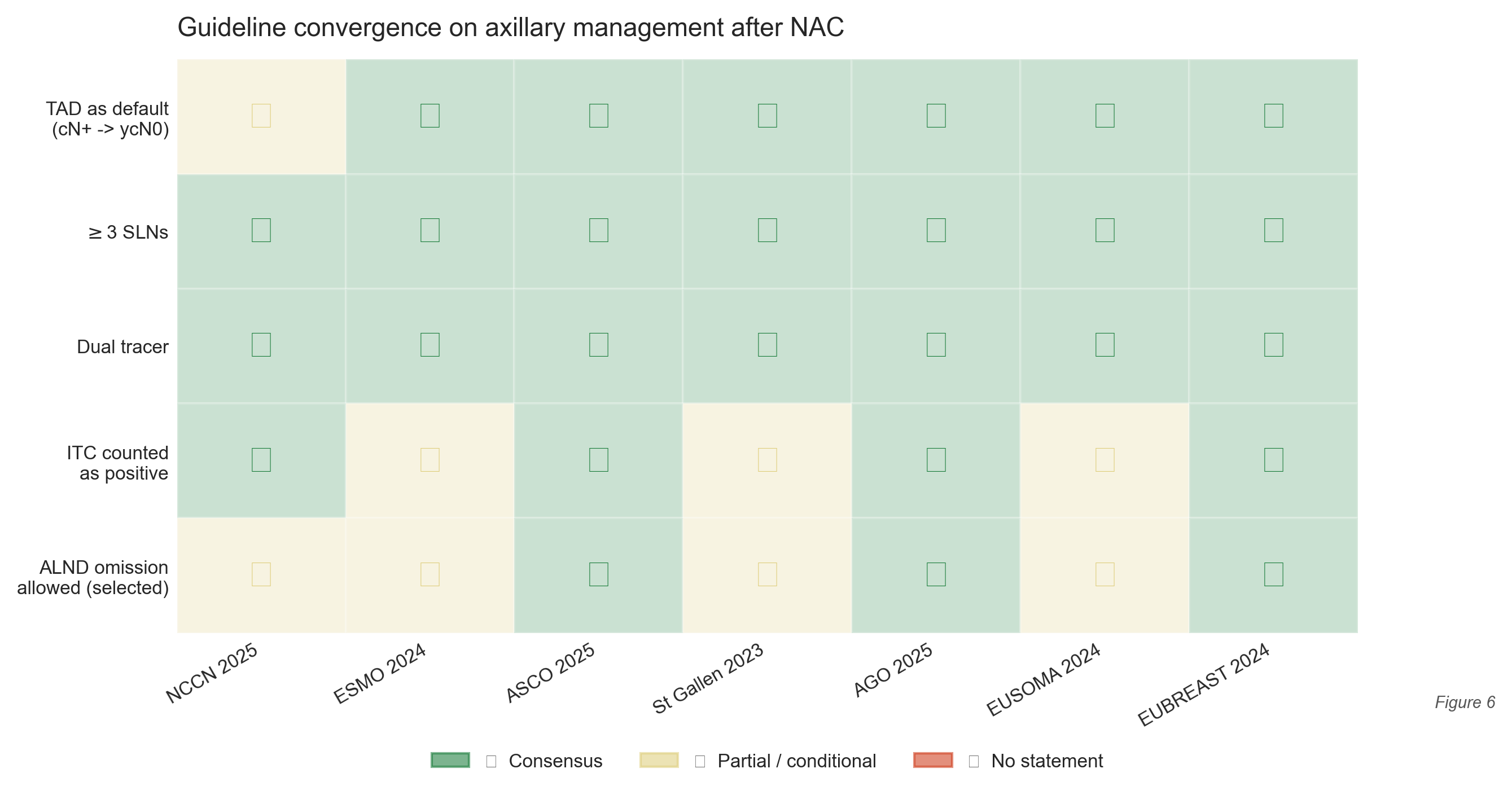
Results. 23 SRs included after PICOS triage (13 ELIGIBLE + 10 BORDERLINE; 10 additional SRs documented as excluded with rationale); ~80,000 unique patients across primary studies. Convergent findings: TAD reduces FNR to <5% (vs 12.6% historical SLNB); molecular subtype is the dominant predictor of ypN0 (HR-/HER2+ 56-72%, TNBC 38-50% chemo-only / >75% chemo-immunotherapy, HR+/HER2- 7-22%); ALND omission in TAD-confirmed ypN0 is supported by NCCN, ESMO, ASCO 2025, St Gallen, AGO, EUSOMA and EUBREAST. Five-year axillary recurrence after omission: 1.0% (95% CI 0.49-2.0%) — Low GRADE certainty. Persistent divergence: ITC handling, FNR threshold, regional radiotherapy in ypN0.
Conclusion. Targeted axillary dissection is the convergent standard for axillary staging in cN+ patients undergoing NAC. Patient selection guided by subtype. The chemo-immunotherapy era and Latin-American populations remain priorities for future research.
Keywords: breast cancer · neoadjuvant chemotherapy · sentinel lymph node biopsy · targeted axillary dissection · ypN0 · umbrella review
Metodología cuádruple
PRISMA 2020
Reporting transparente del proceso de selección y flujo de evidencia. Flow diagram con 5,516 records → 146 únicos → 137 full-text → 33 SRs candidatos → 23 incluidos tras triage PICOS.
AMSTAR-2
Calidad metodológica de cada SR: 16 ítems, 7 críticos. Scoring abstract-based pilot ⇒ 23/23 Critically Low (full-text rescoring planificado).
PICOS triage
Filtro PICOS prospectivo aplicado v1.3 (2026-05-14): 33 SRs candidatos → 13 ELIGIBLE (axila NAC cN+) + 10 BORDERLINE (documentados) + 10 EXCLUDED (linfedema, PRO, reconstructive — rationale en _excluded_after_triage_2026-05-14/).
GRADE
Certainty of evidence por outcome (9 outcomes). Resultado: pCR ⊕⊕⊕○ Moderate · FNR TAD vs SLNB ⊕⊕⊕○ · 5y axillary recurrence ⊕⊕○○ Low · OS ⊕○○○ Very Low.
Figuras editoriales (300 dpi, PNG + TIFF)
Figura 1 · PRISMA 2020 flow
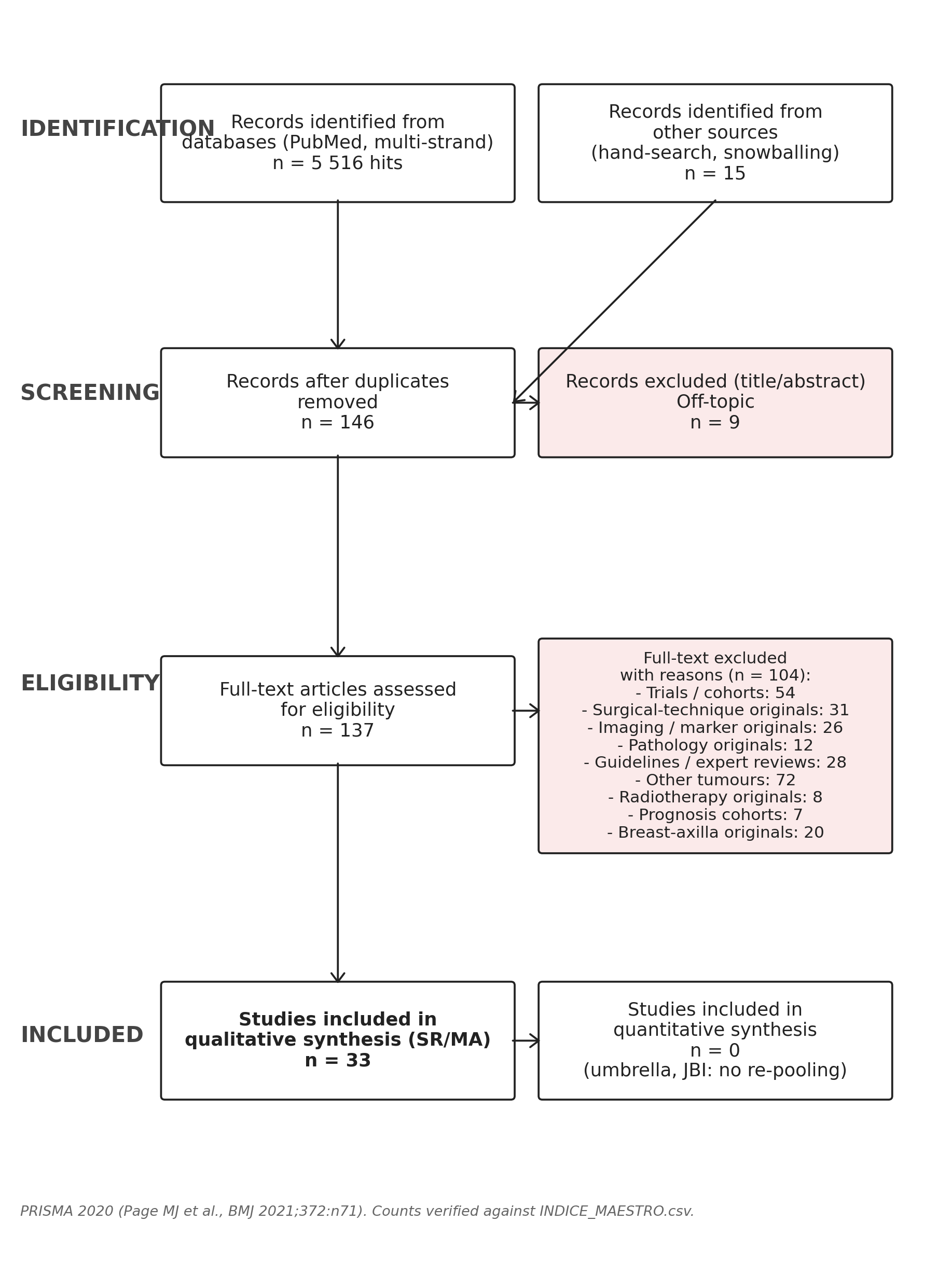
Figura 2 · AMSTAR-2 heatmap
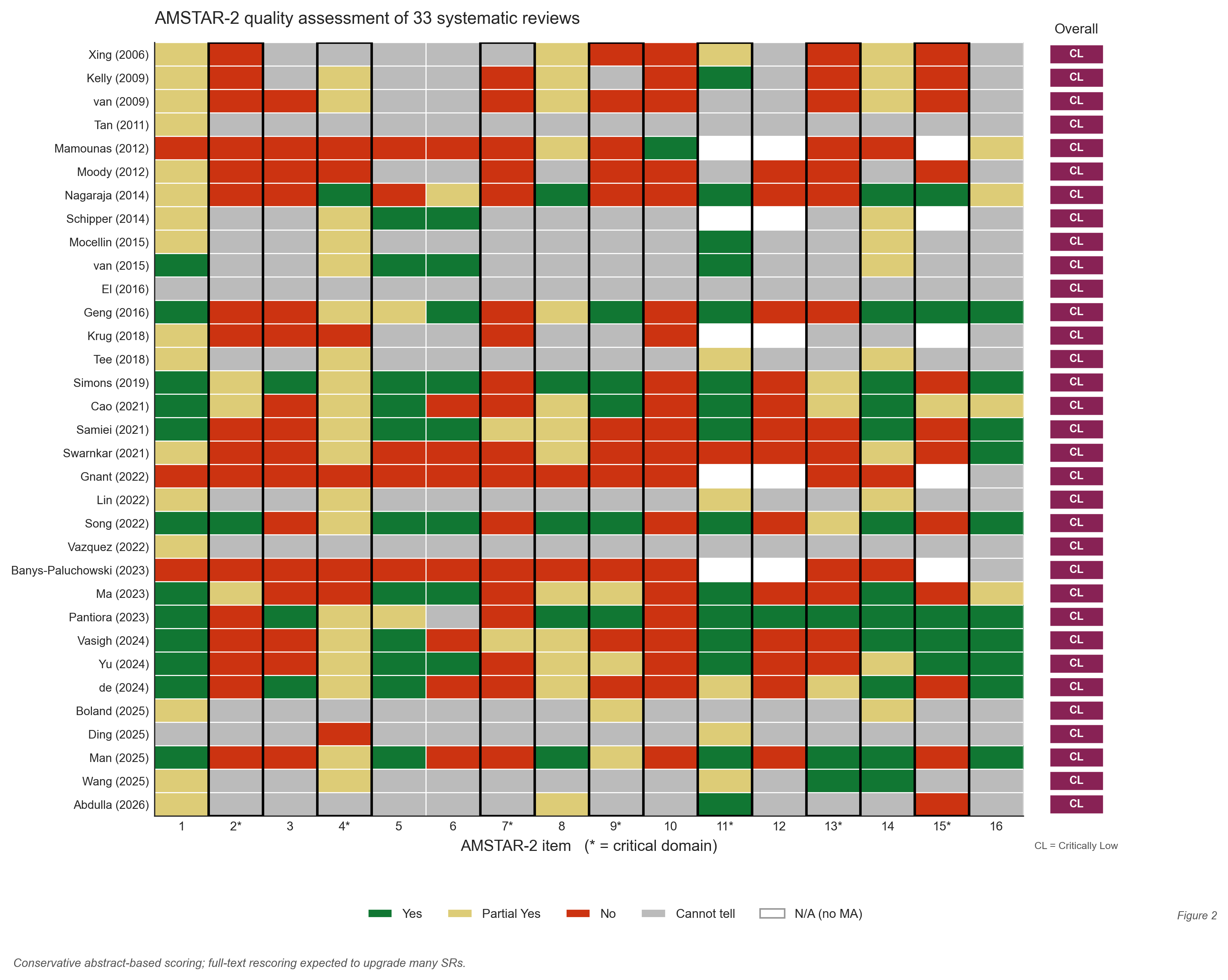
Figura 3 · ypN0 forest por subtipo
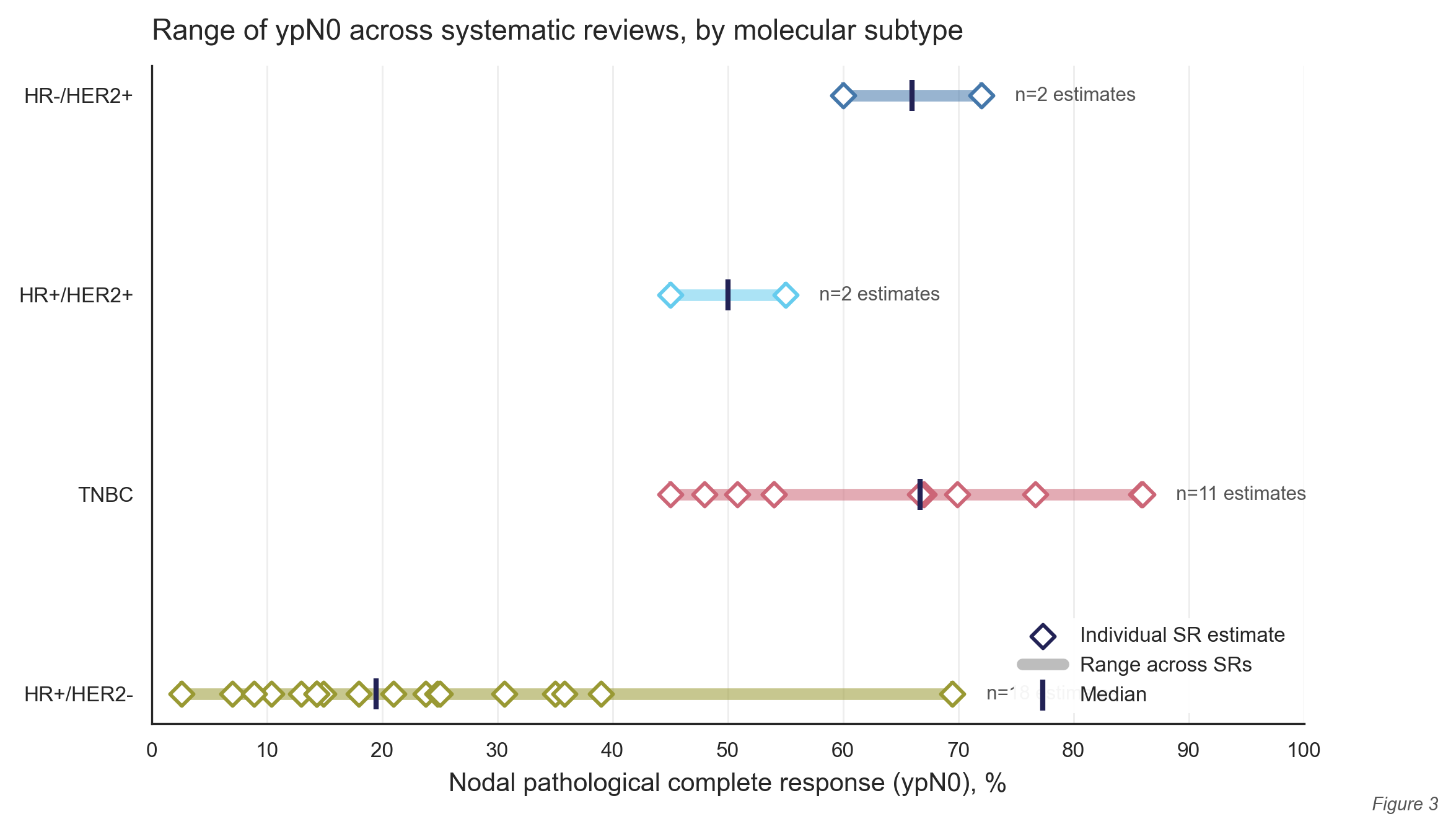
Figura 4 · FNR por técnica
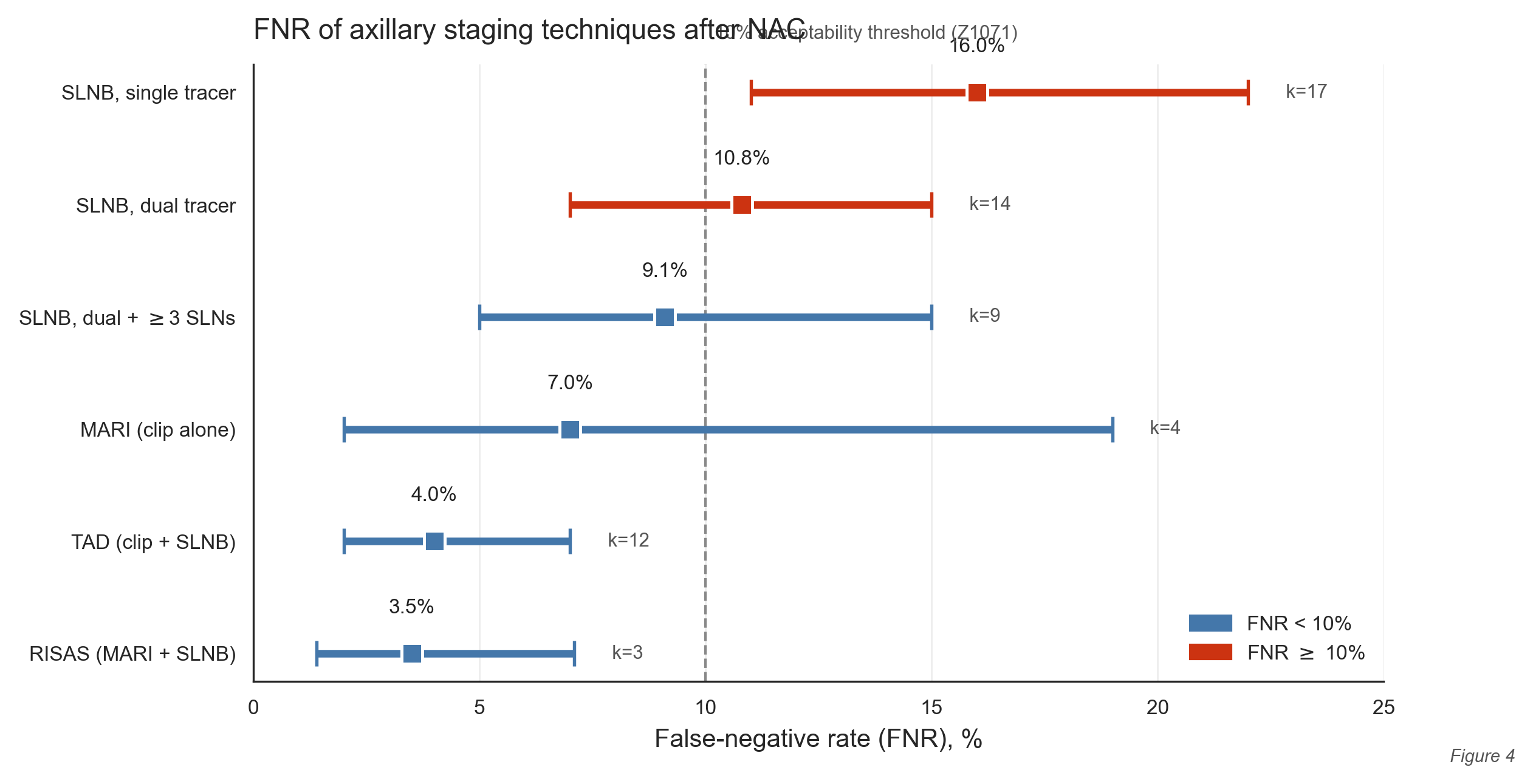
Figura 5 · Timeline 2006-2026
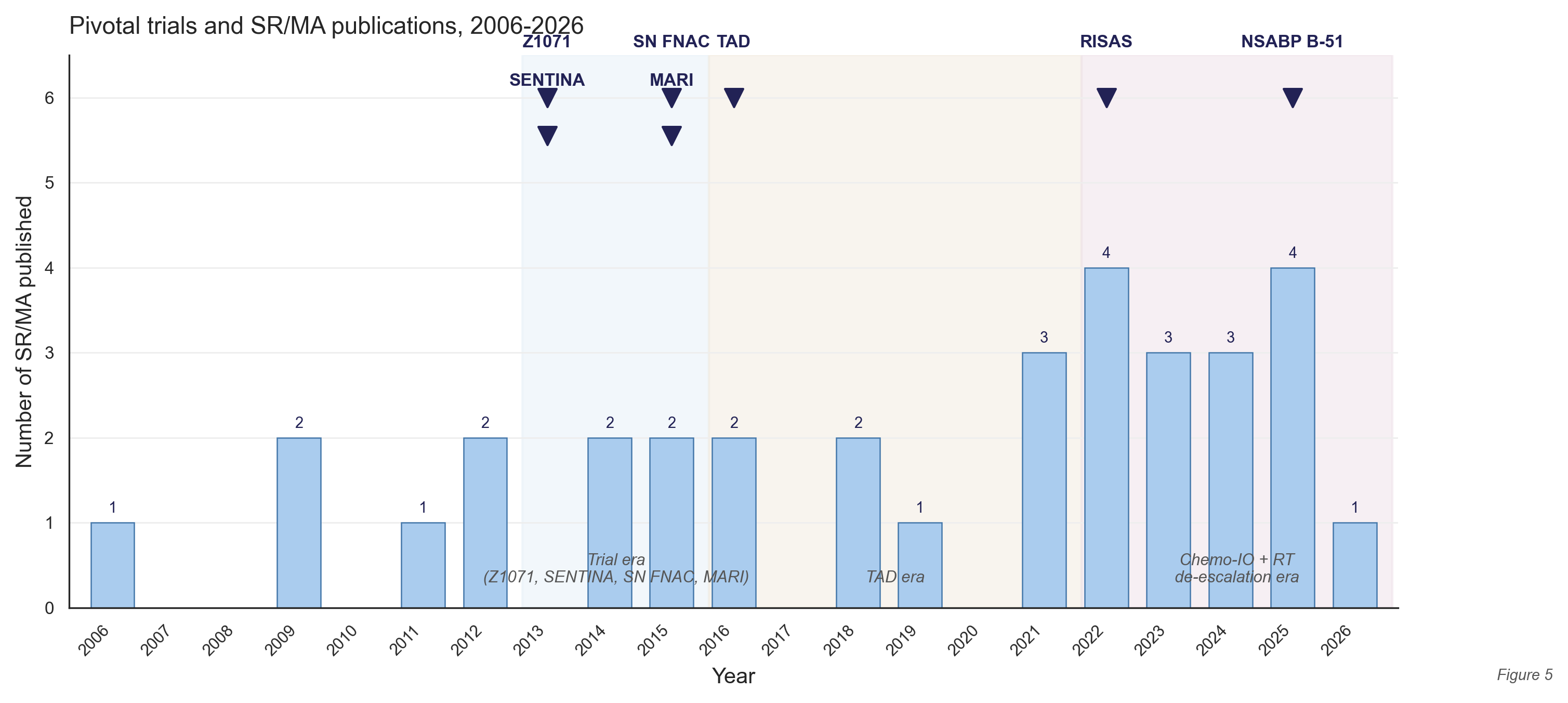
Figura 6 · Convergencia de guías
Bundle del paper (descarga ZIP, 3.3 MB)
paper_umbrella/
├── 01_protocolo/
│ ├── PROSPERO_protocol.md (~3,800 words, 30 sections)
│ ├── PROSPERO_submission_form.txt (copy-paste ready for CRD portal)
│ └── search_strategy_pilot.md (PubMed + EMBASE + Cochrane + Epistemonikos)
│
├── 01b_picos_triage/ (NEW · v1.3 · 2026-05-14)
│ ├── picos_triage_v1.3.md (criteria + decisions)
│ └── _excluded_after_triage_2026-05-14/ (10 SRs · rationale per file)
│
├── 02_amstar2/
│ ├── amstar2_scores.csv (23 SRs × 16 items)
│ ├── amstar2_detailed.md (per-item analysis + Tee 2018 / Simons 2019 anchors)
│ └── score_amstar.py (reproducible Python pipeline)
│
├── 03_prisma/
│ ├── prisma_flow.png (publication-ready 300dpi)
│ ├── prisma_flow_data.md (counts table · 23 included + 10 excluded)
│ ├── prisma_flow.dot/.py (Graphviz + matplotlib renderers)
│ ├── data_extraction_template.md
│ ├── data_extraction_filled.md (23 per-SR cards)
│ └── sr_metadata_extracted.csv
│
├── 04_manuscrito/
│ ├── manuscript.md (~5,400 words, 11 sections)
│ ├── abstract.md (BJS 250w + EJSO 300w)
│ ├── highlights.md (5 Elsevier bullets)
│ ├── grade_assessment.md (~2,200 words, 9 outcomes)
│ ├── grade_table_for_results.md (Table 6 SoF)
│ ├── grade_methods_paragraph.md
│ ├── references.md (90 Vancouver refs)
│ └── tables/ (5 tables ready to insert)
│
├── 05_figuras/ (6 figures × PNG + TIFF + legends)
│ └── make_figures.py (reproducible)
│
├── 06_supplementary/
│ ├── S1_search_strategy.md
│ ├── S2_PRISMA_2020_checklist.md
│ ├── S3_AMSTAR2_full.md
│ ├── S4_excluded_studies.md
│ ├── S5_data_extraction_extended.md
│ ├── S6_glossary.md
│ └── S7_GRADE_summary_of_findings.md
│
└── 07_submission/
├── cover_letter_BJS.md (rank 1 target)
├── cover_letter_EJSO.md (rank 2)
├── cover_letter_TheBreast.md (rank 3, full open access)
├── CRediT_statement.md
├── data_availability.md
├── title_page.md
└── abstract_for_journal_submission.md (250/300 word variants)
Revistas objetivo (cover letters listas)
| Rank | Revista | IF (2024) | OA | Justificación |
|---|---|---|---|---|
| 1 | British Journal of Surgery | ~6.0 | Hybrid | Publicó Xing 2006, Tee 2018, Pantiora 2023, de Wild 2024 (4 SRs del set) |
| 2 | EJSO (Eur J Surg Oncol) | ~3.8 | Hybrid | Audiencia europea de cirugía oncológica; énfasis editorial en de-escalada |
| 3 | The Breast | ~5.7 | Full OA | EUSOMA + EUSOBI + SIS; alineado con filosofía open-tool |
| 4 | Annals of Surgical Oncology | ~4.7 | Hybrid | Backup; visibilidad norteamericana |
| 5 | JAMA Surgery | ~16.0 | Hybrid | Más selectiva; viable si la sección política se enfatiza |
Reviewers sugeridos (en cover letters)
Caudle (MDA) · Kuemmel (German Breast Group) · Boileau (McGill) · Smidt (Maastricht/RISAS) · Banys-Paluchowski (AGO) · Boughey (Mayo) · Mamounas (NSABP) · Weber (EUBREAST) · Rubio (EUSOMA) · Cardoso · Gentilini · Loibl.
📄 Citación sugerida (preprint)
Cervera S, Duque D, et al. Axillary Management After Neoadjuvant Chemotherapy in Node-Positive Breast Cancer: An Umbrella Review of 23 Systematic Reviews and Meta-Analyses (13 ELIGIBLE + 10 BORDERLINE; 2006–2026). Manuscript in preparation. PROSPERO ID-TBD. Available at: https://ganglio.cicatra.com/paper.html
Próximos pasos
- 2026-06: Submit protocol to PROSPERO (form ready in
01_protocolo/) - 2026-07: Full-text rescoring AMSTAR-2 (23 SRs incluidas; anchors Tee 2018 y Simons 2019) — esperamos upgrade de varias a Low/Moderate
- 2026-08: Recruitment de biostatistician + senior breast surgeon como coautores
- 2026-09: Data extraction final + GRADE consolidation post-rescoring
- 2026-10: Internal review + redacción final del manuscrito
- 2026-11: Submission a BJS
- 2027-Q1/Q2: Estimated publication